Impaction is very bad constipation where poo can build up in the abdomen and become immobile in the intestines. The child may pass very small stools every few days or have very infrequent bowel movements. They may have ‘leaks’ of stools causing soiling, where poo has bypassed other hard poo, out of the child’s control (overflow).
Disimpaction means giving laxatives in sufficiently large quantities to ‘clear out’ all accumulated poo. If you give a standard dose of laxative it is likely to soften the poo but not stimulate the bowel to empty fully.
Starting Disimpaction: Age 1 to 4 years
On day 1 take two paediatric sachets, then follow the table below (you may have to turn your phone or tablet sideways to view the full table) until the stools have become loose and watery for at least 24 hours.
| Day |
1 |
2 |
3 |
4 |
5 |
6+ |
| Sachets* |
2 |
4 |
4 |
6 |
6 |
8 |
| Water to Mix (ml) |
125 |
250 |
250 |
375 |
375 |
500 |
Starting Disimpaction: Age 5-11 years
On day 1 take four paediatric sachets, then follow the table below (you may have to turn your phone or tablet sideways to view the full table) until the stools have become loose and watery for at least 24 hours.
| Day |
1 |
2 |
3 |
4 |
5 |
6+ |
| Sachets* |
4 |
6 |
8 |
10 |
12 |
12 |
| Water to Mix (ml) |
250 |
375 |
500 |
625 |
750 |
750 |
Starting Disimpaction: Age over 12 years
Children over 12 years should be treated with an adult preparation – the macrogol is exactly the same but there is twice as much in the sachet. (you may have to turn your phone or tablet sideways to view the full table).
| Day |
1 |
2 |
3 |
4 |
5 |
6+ |
| Sachets* |
4 |
6 |
8 |
8 |
8 |
8 |
| Water to Mix (ml) |
500 |
750 |
1000 |
1000 |
1000 |
1000 |
* Number of sachets per day, taken over a 12 hour period
When is disimpaction achieved?
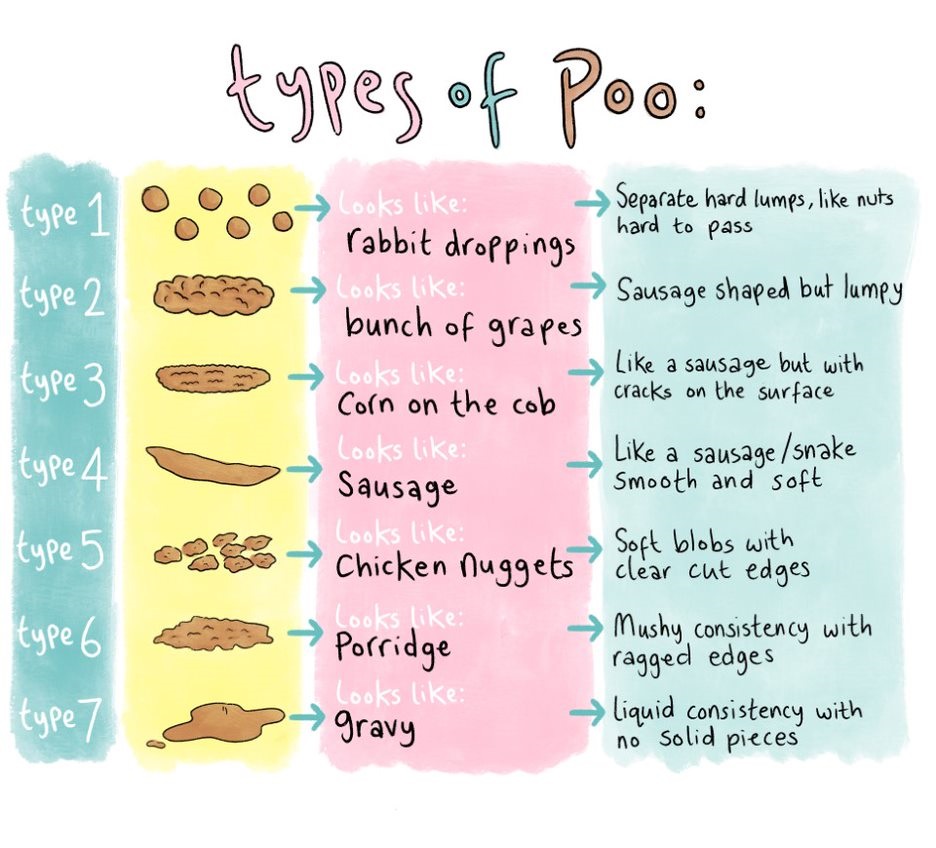
When your child’s poo has the appearance of brown bitty water (type 7 on the stool chart) on at least one occasion, the disimpaction regime can be stopped. It is normal for this to take 7 to 14 days. Laxative treatment does need to continue to prevent recurrence of constipation, and the allow the stretched bowel to regain its tone. If it takes longer than 14 days, make an appointment to see your child’s GP.
Maintenance dose
Your child should be given a maintenance dose of their laxative after disimpaction. The dose should be adjusted to ensure your child poos at least one soft poo every day. You will therefore need to monitor their poos and increase/decrease laxative doses accordingly. Your child may need to stay on laxatives for many months or even years. You will know if they need less laxatives – check their poo and
decrease the dose if it is too sloppy.
| Age |
Quantity |
| 1 -5 years |
½ - 3 sachets/day |
| 5-12 years |
1-4 sachets/day |
| Over 12 years |
1-2 adult sachets/day |
Maintenance
Once disimpaction is achieved, reduce the number of sachets to a maintenance dose. This will be half the disimpaction dose, taken over a 12 hour period, up to a maximum of 4 paediatric sachets per day. Over time, it should be possible to reduce the maintenance dose, aiming for type 3-4 stools, but be aware this can take months to achieve. It is likely that is the sachets are stopped too soon that constipation may return and we would advise continuing a maintenance dose for at least 6 months.